Fill Out Your DD 2870 Template
The DD 2870 form plays a crucial role in the world of military healthcare and benefits. It serves as a request for the release of medical records, ensuring that service members and their families can access vital health information when needed. Completing this form is often necessary for those seeking treatment or benefits, as it allows healthcare providers to share pertinent medical history with authorized parties. The form is straightforward, but it requires careful attention to detail, including the correct identification of the individual requesting the records. Additionally, understanding the privacy implications is essential, as the form involves sensitive personal health information. By navigating the process of completing the DD 2870, individuals can better manage their healthcare needs and ensure that they receive the support they deserve.
Similar forms
The DD Form 214 is a document that serves as a certificate of release or discharge from active duty in the U.S. Armed Forces. Like the DD 2870, which is used for requesting medical records, the DD 214 provides essential information about a service member’s military history. It includes details such as the duration of service, type of discharge, and any awards received. Both forms are crucial for veterans when applying for benefits or verifying their military service.
The Standard Form 180 (SF 180) is another document that shares similarities with the DD 2870. This form is used to request military records from the National Archives and Records Administration. Just as the DD 2870 facilitates access to specific medical records, the SF 180 allows individuals to obtain various military documents, including service records and discharge papers. Both forms require personal information and details about the service member to process the request efficiently.
The Privacy Act Statement is a document that outlines how personal information is collected, used, and protected by federal agencies. While the DD 2870 focuses on the request for medical records, the Privacy Act Statement ensures that individuals understand their rights regarding their personal data. Both documents emphasize the importance of privacy and informed consent when handling sensitive information related to military service and health records.
When dealing with property transfers in Illinois, it's essential to understand the significance of legal documents like a Quitclaim Deed. This form can be particularly useful for individuals wishing to establish ownership without warranties, such as in family transactions or when resolving title issues. If you're ready to begin the process, you can find more information and access the necessary forms here: https://quitclaimdeedtemplate.com/illinois-quitclaim-deed-template/.
The VA Form 21-526EZ is a claim form for veterans seeking disability compensation or pension benefits from the Department of Veterans Affairs. Similar to the DD 2870, which is used to request medical records for treatment verification, this form requires detailed information about the veteran’s service and medical history. The connection lies in the fact that both forms aim to assist veterans in accessing necessary resources and benefits related to their military service.
The Form 10-5345 is utilized by veterans to request access to their health information from the Department of Veterans Affairs. This form bears resemblance to the DD 2870 in that both are designed to facilitate the sharing of medical records. They require the individual’s consent and specific details to ensure that the requested information is accurately provided, highlighting the importance of authorization in accessing personal health records.
The Form 1172-2 is a document used to apply for a military identification card. While it serves a different purpose than the DD 2870, both forms require personal information and proof of eligibility. The DD 2870 is focused on medical records, while the Form 1172-2 is concerned with identification. However, both documents are essential for ensuring that service members and their families receive the benefits and services they are entitled to.
Form Specifications
| Fact Name | Description |
|---|---|
| Purpose | The DD 2870 form is used to authorize the release of medical and dental records for military personnel and their dependents. |
| Who Uses It | This form is primarily used by service members, veterans, and their family members seeking access to their health records. |
| Submission Process | Individuals must complete the form and submit it to the appropriate military health facility or records office. |
| Privacy Considerations | The form includes provisions to protect the privacy of the individual’s health information in accordance with federal laws. |
| State-Specific Forms | Some states may have their own versions or additional requirements for releasing medical records, governed by state laws such as HIPAA. |
| Validity | The DD 2870 form does not expire, but it must be filled out correctly to be considered valid for the release of records. |
Different PDF Templates
Pay Stub for Contractor - Streamlines the invoicing process for independent contractors.
When buying or selling a motorcycle in Colorado, it's crucial to have the proper documentation in place. The Colorado Motorcycle Bill of Sale form serves this purpose by ensuring all transaction details are clearly recorded, preventing any misunderstandings between the buyer and seller. For those looking to simplify the process, you can easily access a suitable template through Colorado PDF Forms, making ownership transfer seamless and efficient.
Download D1 Form Pdf - Applicants must ensure that all information is consistent and truthful to avoid delays.
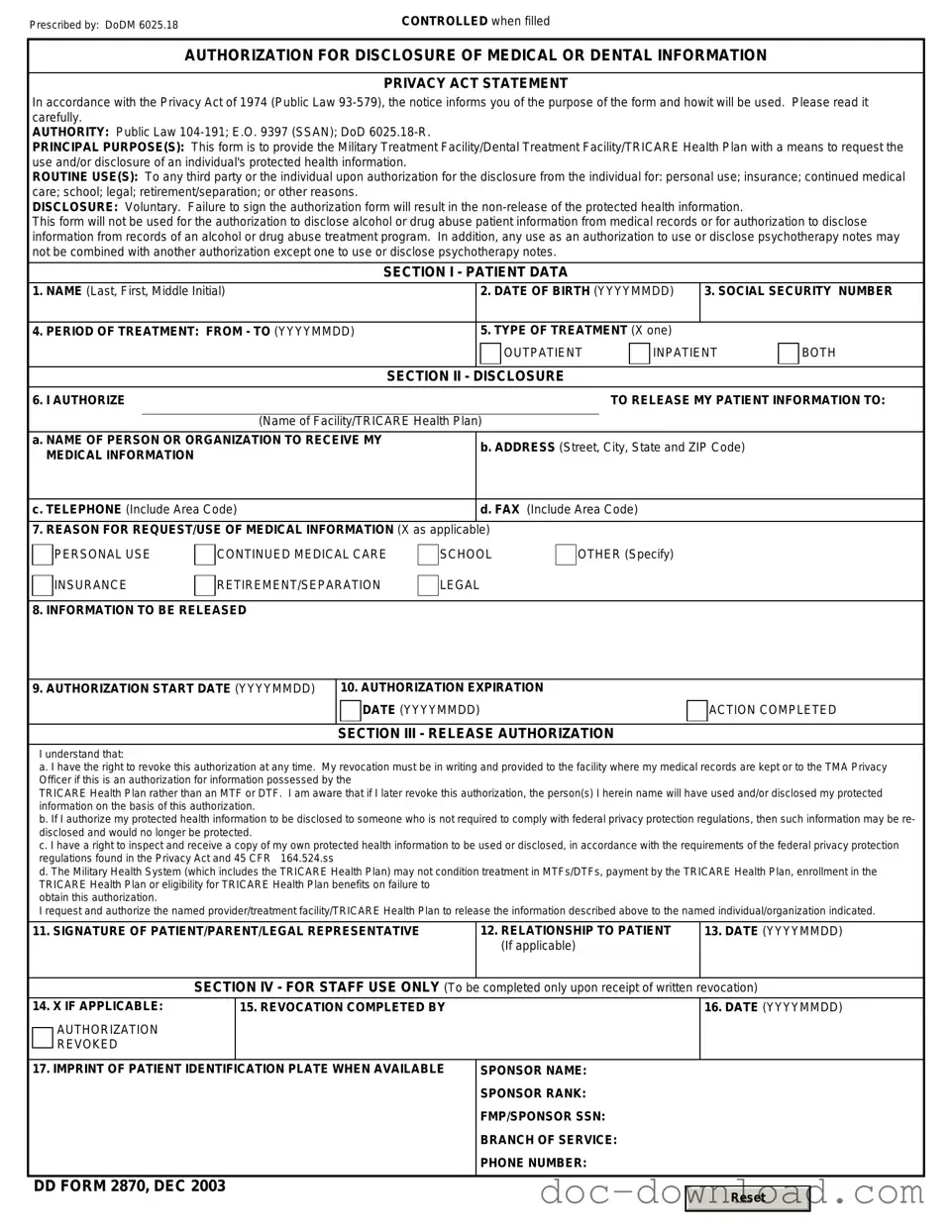
Sample - DD 2870 Form
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|