Fill Out Your Annual Physical Examination Template
The Annual Physical Examination form serves as a crucial tool for both patients and healthcare providers, ensuring a comprehensive overview of an individual's health status. This form is divided into two main parts, each designed to gather essential information that will facilitate a thorough medical evaluation. In the first part, patients are required to provide personal details such as their name, date of birth, and address, along with a summary of their medical history, current medications, and any allergies or sensitivities. This section also includes vital information about immunizations, tuberculosis screening, and any past hospitalizations or surgical procedures. The second part focuses on the general physical examination, where healthcare professionals will document vital signs, assess various body systems, and note any abnormalities. Additionally, there is space for recommendations regarding health maintenance, dietary guidelines, and potential limitations on activities. By completing this form accurately and thoroughly, patients help ensure that their healthcare providers have the necessary information to deliver the best possible care.
Similar forms
The Annual Health Assessment form is similar to the Patient Intake Form. Both documents gather essential information about the patient's medical history and current health status. They typically require personal details such as name, date of birth, and contact information. The Patient Intake Form also includes sections for current medications and allergies, which align closely with the Annual Physical Examination form's requirements for medication and allergy information.
Another comparable document is the Medical History Questionnaire. This form focuses on the patient’s past medical conditions and family history. Like the Annual Physical Examination form, it seeks to identify significant health issues and chronic conditions. Both documents aim to provide healthcare providers with a comprehensive view of the patient’s health to facilitate informed decision-making during medical evaluations.
The Immunization Record is another document that shares similarities with the Annual Physical Examination form. Both forms track vaccination history, ensuring that patients receive necessary immunizations. The Annual Physical Examination form specifically lists required immunizations, while the Immunization Record provides a detailed history of all vaccinations administered, including dates and types of vaccines.
The Lab Test Requisition Form also bears resemblance to the Annual Physical Examination form. Both documents may include sections for ordering specific tests and recording results. The Annual Physical Examination form outlines various tests that may be recommended during the examination, while the Lab Test Requisition Form focuses specifically on laboratory tests that need to be conducted.
The Health Risk Assessment form aligns closely with the Annual Physical Examination form in its purpose to evaluate a patient’s overall health. Both documents assess lifestyle factors, medical history, and current health status. The Health Risk Assessment often includes questions about diet, exercise, and personal habits, similar to the health maintenance recommendations found in the Annual Physical Examination form.
To facilitate the transfer of property ownership in Florida, one can utilize the quitclaimdeedtemplate.com/florida-quitclaim-deed-template/, which provides essential guidance on completing this vital legal document effectively.
The Medication Reconciliation Form is another document that shares a purpose with the Annual Physical Examination form. Both forms aim to ensure that healthcare providers have an accurate list of the patient’s medications. The Annual Physical Examination form includes a section for current medications, while the Medication Reconciliation Form specifically addresses any changes in medications, dosages, or new prescriptions.
The Consent for Treatment form is also similar to the Annual Physical Examination form in that it is often completed prior to a medical appointment. Both documents require patient information and aim to ensure that patients understand the procedures they are consenting to. The Consent for Treatment form specifically addresses patient agreement to medical care, while the Annual Physical Examination form focuses on gathering necessary health information.
The Follow-Up Care Plan is another document that resembles the Annual Physical Examination form. Both forms outline recommendations for ongoing health management after an examination. The Follow-Up Care Plan typically includes specific instructions for further testing or treatment, similar to the recommendations provided in the Annual Physical Examination form.
Lastly, the Emergency Contact Form shares similarities with the Annual Physical Examination form. Both documents require personal information and may include details about the patient’s health status. The Emergency Contact Form focuses on who should be contacted in case of an emergency, while the Annual Physical Examination form emphasizes the patient's health history and current conditions that may be relevant in an emergency situation.
Form Specifications
| Fact Name | Details |
|---|---|
| Purpose | The Annual Physical Examination form is designed to gather essential health information prior to a medical appointment. |
| Required Information | Patients must complete all sections, including personal details, medical history, and current medications, to avoid delays. |
| Immunization Records | Patients are required to provide information on immunizations, including dates and types administered, to ensure comprehensive care. |
| Health Screenings | Various health screenings, such as TB tests and cancer screenings, are included to assess the patient's overall health status. |
| Medication Management | Patients must list current medications, including dosages and prescribing physicians, to facilitate accurate treatment planning. |
| Legal Compliance | In many states, the form must comply with healthcare regulations, such as HIPAA, to protect patient privacy. |
| Emergency Information | The form includes a section for critical information pertinent to diagnosis and treatment in case of an emergency. |
| Physician’s Verification | At the end of the form, the physician must sign and date it, confirming the information provided during the examination. |
Different PDF Templates
Trader Joes - Knowledgeable about health and wellness food options.
In addition to ensuring a smooth transaction, utilizing a Colorado Horse Bill of Sale form provides peace of mind for both the buyer and seller, as it clearly outlines the terms of the sale. For those looking to obtain this vital document, the Colorado PDF Forms offer a convenient resource to complete the necessary paperwork and facilitate the ownership transfer with confidence.
Minor Travel Consent Letter - To participate in many programs, submitting the NCL Parental Consent form is often mandatory.
Roof Condition Certification Form - This record helps maintain transparency between all parties involved.
Sample - Annual Physical Examination Form
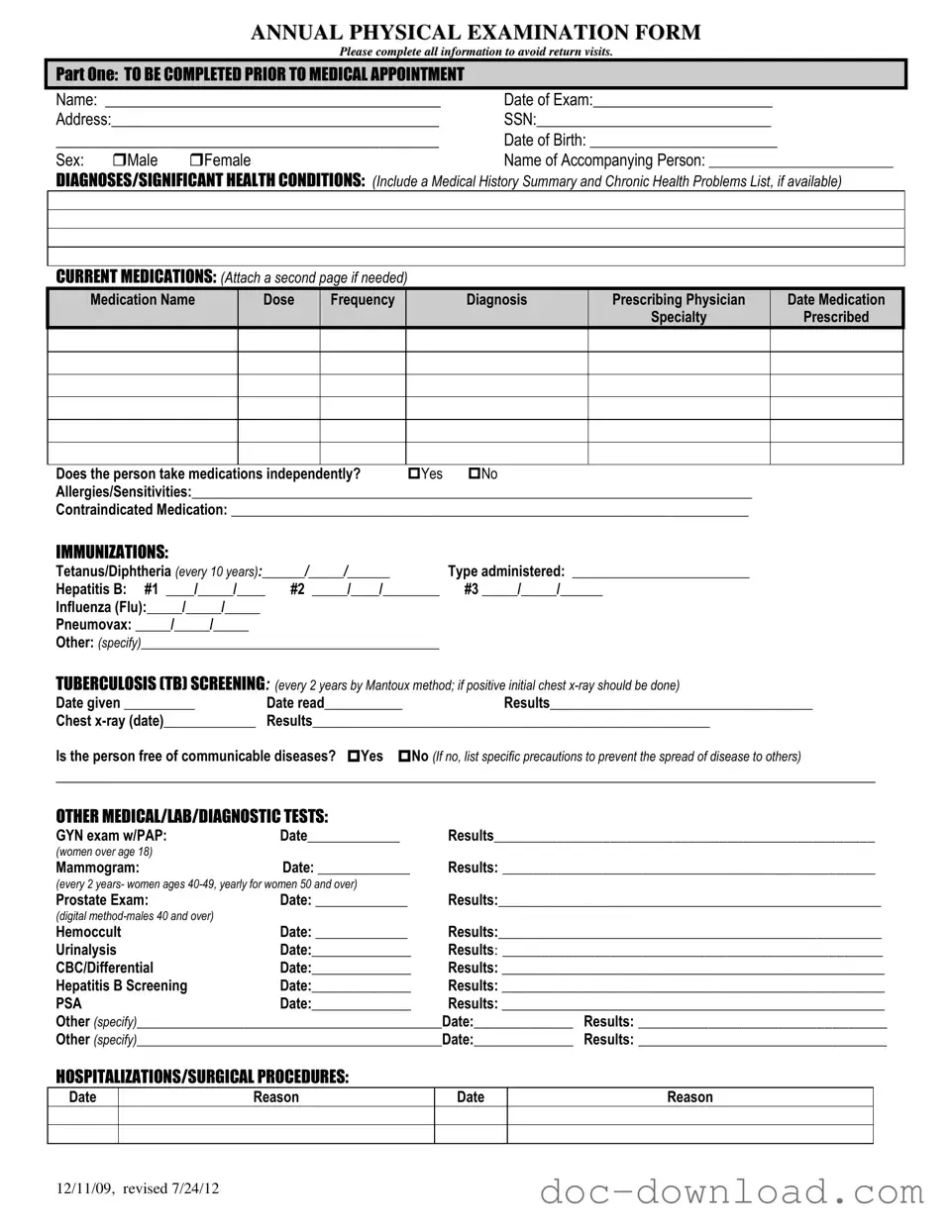
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12
PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
