Fill Out Your Advance Beneficiary Notice of Non-coverage Template
The Advance Beneficiary Notice of Non-coverage (ABN) form plays a crucial role in the Medicare system, particularly for beneficiaries who may be receiving services that Medicare does not cover. This form serves as a notification to patients, informing them that certain items or services may not be reimbursed by Medicare. It is essential for healthcare providers to issue the ABN when they believe that the service provided is not considered medically necessary under Medicare guidelines. By signing the ABN, beneficiaries acknowledge that they understand the potential financial responsibility they may incur for the service in question. The form also outlines the reasons for non-coverage, allowing beneficiaries to make informed decisions regarding their healthcare. Additionally, the ABN includes important information about the appeal process should the beneficiary wish to contest the non-coverage decision. Understanding the implications of the ABN is vital for Medicare recipients to navigate their healthcare options effectively and to avoid unexpected out-of-pocket expenses.
Similar forms
The Advance Beneficiary Notice of Non-coverage (ABN) is similar to the Medicare Summary Notice (MSN). Both documents serve to inform beneficiaries about their Medicare coverage. The MSN provides a summary of services received and indicates which services were covered or denied. In contrast, the ABN is specifically used to notify beneficiaries before they receive services that may not be covered, allowing them to make informed decisions about their care and potential costs.
Another document that shares similarities with the ABN is the Notice of Exclusion from Medicare Benefits (NEMB). The NEMB is issued when a service is not covered by Medicare, but it differs from the ABN in that it is provided after the service has been rendered. While the ABN allows beneficiaries to consent to pay for a service upfront, the NEMB informs them post-service about the lack of coverage, highlighting the importance of both documents in managing beneficiaries' expectations regarding Medicare benefits.
The Explanation of Benefits (EOB) is another document that resembles the ABN. Like the ABN, the EOB informs beneficiaries about their healthcare services and the costs associated with them. However, the EOB is typically issued by private insurance companies rather than Medicare. It details what services were provided, the amount billed, and what the insurance plan covered. Both documents emphasize the financial implications of healthcare services, empowering beneficiaries to understand their responsibilities.
The Prior Authorization Request form is also similar to the ABN in that it involves pre-approval for services. Before certain services are provided, healthcare providers may need to obtain prior authorization from Medicare or another insurer. The ABN serves as a notification that a service may not be covered, while the Prior Authorization Request seeks to confirm coverage before the service is rendered. Both documents play a crucial role in ensuring that beneficiaries are aware of potential costs before receiving care.
The Informed Consent form bears resemblance to the ABN as well. Informed Consent is used in medical settings to ensure that patients understand the risks and benefits of a procedure or treatment. While the ABN focuses on coverage issues, the Informed Consent form emphasizes patient awareness and agreement regarding medical interventions. Both documents prioritize patient autonomy and informed decision-making, ensuring individuals have the necessary information to proceed with their healthcare choices.
The Advance Beneficiary Notice of Non-coverage (ABN) serves as a crucial document for Medicare beneficiaries. It informs patients when a service may not be covered by Medicare. Similarly, the Informed Consent form provides essential information and ensures that patients understand the risks and benefits before undergoing a procedure. Both documents prioritize patient awareness, promoting informed decision-making regarding healthcare options. For those managing their legal affairs in Georgia, resources like Georgia PDF Forms can be invaluable.
The Patient Responsibility Agreement is another document that aligns with the ABN. This agreement outlines the financial responsibilities of the patient regarding services received, particularly when there is uncertainty about coverage. Similar to the ABN, it helps patients understand their potential out-of-pocket costs before receiving care. Both documents aim to clarify financial obligations, reducing confusion and promoting transparency in the healthcare process.
Lastly, the Cost Estimate form is akin to the ABN in that it provides patients with an estimate of potential charges for medical services. This document is often used by healthcare providers to give patients a clearer picture of what to expect financially before treatment. While the ABN indicates that a service may not be covered by Medicare, the Cost Estimate form helps patients anticipate their expenses. Both documents facilitate informed decision-making and enhance the patient experience by addressing financial concerns upfront.
Form Specifications
| Fact Name | Description |
|---|---|
| Purpose | The Advance Beneficiary Notice of Non-coverage (ABN) informs Medicare beneficiaries that a service may not be covered. |
| When to Use | Providers should issue an ABN when they believe that Medicare may deny payment for a service or item. |
| Beneficiary Rights | Beneficiaries have the right to refuse services after receiving an ABN, knowing they may have to pay out-of-pocket. |
| Delivery Method | The ABN can be delivered in person, by mail, or electronically, as long as the beneficiary receives it before the service. |
| Signature Requirement | Beneficiaries must sign the ABN to acknowledge understanding of potential non-coverage. |
| State Variations | Some states may have additional forms or requirements regarding notice of non-coverage, governed by state-specific laws. |
| Not a Guarantee | Signing an ABN does not guarantee that the service will be paid for by Medicare; it merely indicates potential non-coverage. |
| Effective Communication | Clear communication is crucial; providers must explain the reason for the ABN to the beneficiary. |
| Timeframe | Providers should issue the ABN as soon as they suspect non-coverage, ideally before the service is provided. |
| Documentation | Providers must keep a copy of the signed ABN in the beneficiary's medical record for future reference. |
Different PDF Templates
Vtr-40 Odometer Disclosure Statement - Both seller and buyer must be honest to avoid complications.
CBP Form 6059B - Travelers may be asked to provide additional documentation along with this form.
For those seeking to formalize rental agreements, a well-prepared document can simplify the process; consider using a comprehensive guide on how to create a Lease Agreement that meets your specific needs. For further details, explore our fillable templates available at the fillable Lease Agreement form.
Imm1294e - Applicants must provide their passport information including number, issuance date, and expiration date.
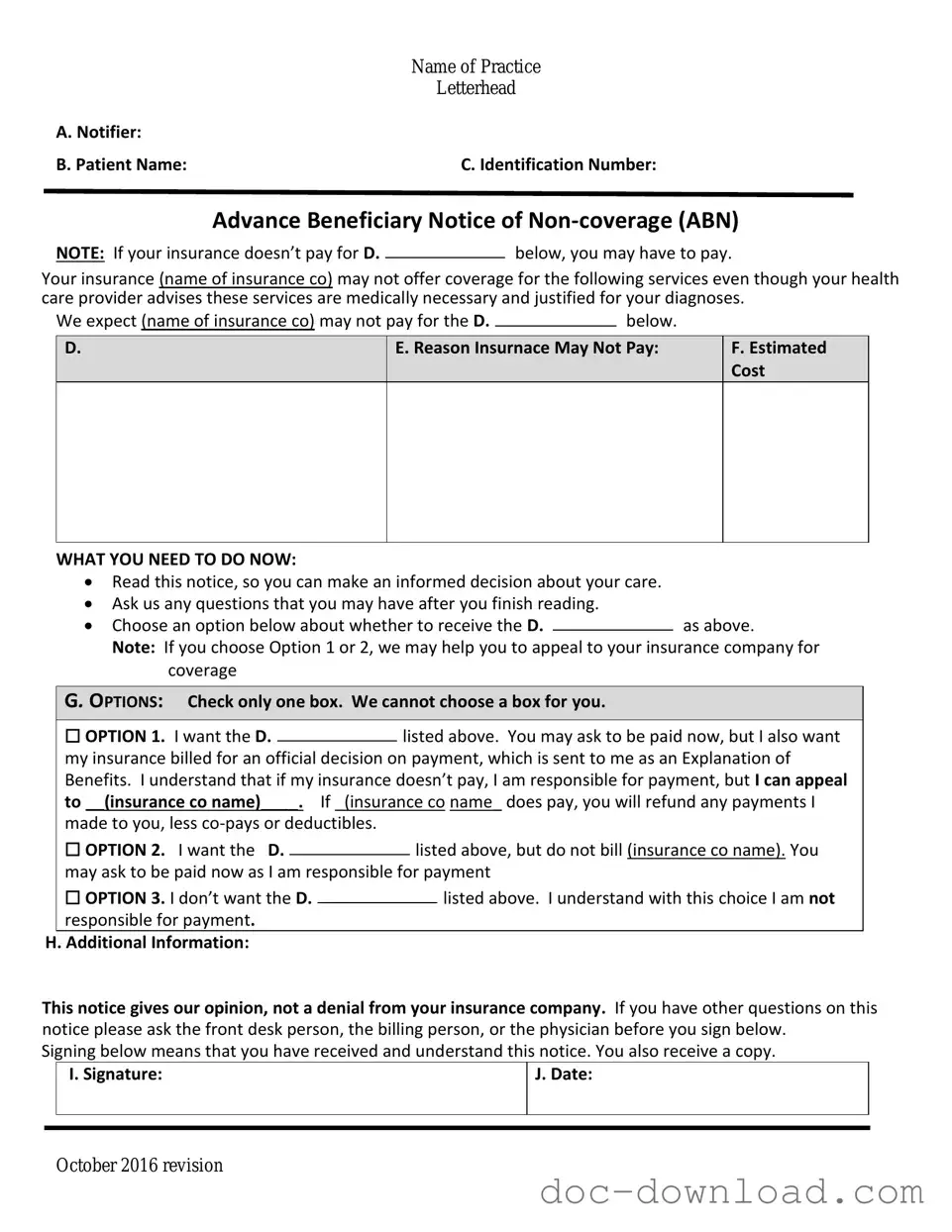
Sample - Advance Beneficiary Notice of Non-coverage Form
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision